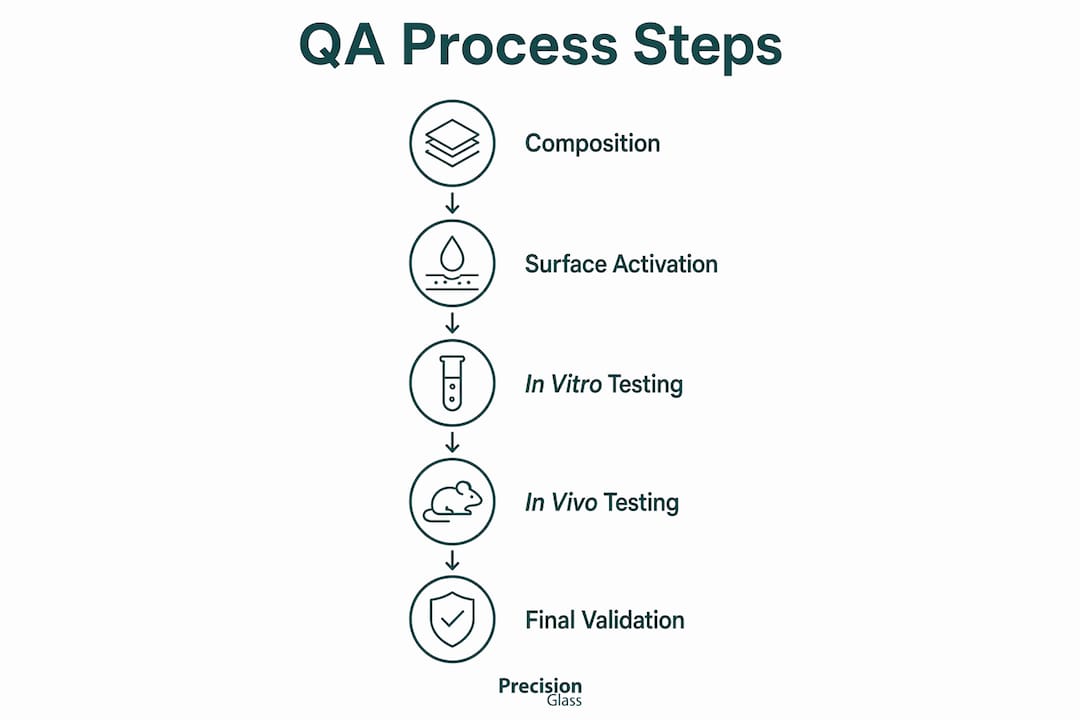
Biocompatible glass is defined as any glass material that performs its intended function without triggering harmful biological responses in the surrounding tissue or fluid environment. Knowing how to ensure biocompatible glass is not optional for quality assurance specialists in medical device or industrial manufacturing. It requires a structured, multi-stage validation process covering material composition, surface treatment, and biological testing under both ISO 10993 and ASTM F756 frameworks. The process begins with selecting the right glass formulation, moves through in vitro cytotoxicity screening, and concludes with in vivo confirmation in relevant biological models. Each stage builds on the last, and skipping any one of them creates compliance gaps that regulators will find.
What are the prerequisites for ensuring biocompatible glass?
The foundation of biocompatibility in glass materials is composition. Not all glass formulations behave the same way in biological environments. Borosilicate glass, aluminosilicate glass, and bioactive glass variants such as 45S5 each carry different ion release profiles, surface chemistries, and degradation rates. Selecting the wrong base composition before testing begins wastes time and resources.
Glass composition directly controls biological response. Research shows that mild alkaline glass microenvironments promote osteogenic differentiation and inhibit osteoclastic activity, which matters significantly in bone regeneration applications. A containerless melting process yields a stable network structure with a reduced ion release rate, improving overall compatibility. Equally, dopant concentration adjustments in formulations such as 45S5 bioactive glass doped with samarium demonstrate that even minor compositional changes shift the balance between biocompatibility and antimicrobial performance.
Before any biological testing begins, quality assurance teams need the following in place:
- Glass composition documentation: Full elemental analysis and network modifier ratios confirmed against specification
- Surface treatment materials: Plasma activation equipment and medical-grade hydrophilic polymers including PVP, PAAm, and zwitterionic polymer solutions
- Laboratory equipment: UV-Vis spectrophotometer for MTT absorbance readings, LDH activity kits, fluorescence microscope for morphological assessment
- Cell lines: L929 fibroblasts for general cytotoxicity, MG-63 or SaOS-2 osteoblast-like cells for bone-contact applications
- Regulatory frameworks: ISO 10993-5 for cytotoxicity, ISO 10993-6 for implantation, and ASTM F756 for haemolysis testing
The table below summarises the key cell lines and their appropriate application contexts:
| Cell line | Application context | Key metric assessed |
|---|---|---|
| L929 (mouse fibroblast) | General cytotoxicity screening | Cell viability, morphology |
| MG-63 (osteoblast-like) | Bone-contact devices | Proliferation, differentiation |
| SaOS-2 (osteosarcoma) | Mineralisation studies | Alkaline phosphatase activity |
Selecting the correct cell line before testing begins prevents mismatched results that cannot be used for regulatory submissions. Matching cell biology to the intended clinical application is a prerequisite, not an afterthought. You can find further guidance on types of medical glass and their procurement considerations through Precision Glasses.
How to conduct in vitro testing to verify glass biocompatibility
In vitro testing is the primary screening stage for biocompatible glass testing methods. The two most widely used assays are the MTT assay, which measures mitochondrial metabolic activity as a proxy for cell viability, and the LDH assay, which quantifies membrane damage by detecting lactate dehydrogenase released from lysed cells. Standardised cytotoxicity testing evaluates cell viability at 24 and 48 hours post-exposure using these cell lines, giving a time-resolved picture of material toxicity.
The standard testing sequence runs as follows:
- Prepare glass extracts or direct contact specimens according to ISO 10993-12 extraction ratios (typically 3 cm² per mL or 0.1 g per mL).
- Seed the selected cell line at a standardised density and allow 24 hours for attachment before exposure.
- Apply the glass extract or place the glass specimen in direct or indirect contact with the cell monolayer.
- Incubate at 37°C in 5% CO₂ for 24 hours, then repeat the measurement at 48 hours.
- Run the MTT assay by adding the tetrazolium reagent, incubating for 4 hours, then dissolving formazan crystals and reading absorbance at 570 nm.
- Run the LDH assay on the culture supernatant to confirm membrane integrity data independently of the MTT result.
- Perform fluorescence microscopy to assess cell morphology, adhesion, and any signs of apoptosis or necrosis.
- Compare all results against positive and negative controls to calculate percentage viability relative to untreated cells.
One critical variable that many QA protocols underestimate is the choice between static and dynamic testing conditions. Dynamic testing better simulates physiological fluid flow and produces measurably different ion release and bioactivity outcomes compared to static immersion. Static tests are faster and cheaper, but they overestimate ion accumulation at the glass surface and can produce false-positive cytotoxicity signals in soluble glass systems.
Pro Tip: Multi-parametric testing combining MTT, LDH, and fluorescence microscopy in parallel reduces false positives and false negatives. A single assay result should never be used as the sole basis for a biocompatibility pass or fail decision.

What surface treatment processes improve glass biocompatibility?
Glass is chemically inert by nature. That inertness protects it from corrosion, but it also makes it difficult to bond coatings reliably. Without surface modification, hydrophilic coatings applied to glass substrates delaminate under mechanical stress or fluid exposure, which is a direct failure mode in medical device applications.
Plasma treatment is the most reliable method for surface activation. It generates reactive hydroxyl groups on the glass surface by exposing it to oxygen or argon plasma for a controlled duration. These hydroxyl groups form covalent bonds with coating polymers, dramatically increasing adhesion strength and resistance to delamination. Plasma activation is the critical step that prevents coating failure in biological environments.
Once the surface is activated, the appropriate hydrophilic coating polymer is selected based on the application:
- PVP (polyvinylpyrrolidone): High lubricity, widely used in catheter and guidewire applications, good wettability in aqueous environments
- PAAm (polyacrylamide): Strong anti-biofouling performance, suited to diagnostic device surfaces where protein adsorption must be minimised
- Zwitterionic polymers: Excellent thromboresistance and long-term stability, preferred for blood-contacting glass components
Each of these polymers contributes to biocompatibility in glass materials by reducing protein adsorption, preventing platelet activation, and lowering the risk of tissue trauma during device insertion or use. Hydrophilic polymer coatings improve lubricity, wettability, and anti-biofouling performance in biological environments. The practical implication is that coating selection cannot be separated from surface preparation. One without the other produces unreliable results.
Pro Tip: Always perform surface characterisation using contact angle measurement and X-ray photoelectron spectroscopy (XPS) before applying any coating. Contact angle below 20° confirms adequate hydroxyl group density for reliable polymer adhesion. Skipping this step is the most common cause of coating failure in production.
Precision Glasses applies glass fabrication processes that include surface priming and plasma activation as standard steps in medical and technical glass production.
How to validate biocompatibility through in vivo testing
In vitro data confirms that a glass material is not acutely toxic to cells under controlled conditions. It does not confirm that the material performs safely inside a living biological system over weeks or months. In vivo testing on large animal models is the required next step for clinical safety confirmation, evaluating long-term tissue integration and functional compatibility before any human use.
The in vivo validation process for biocompatible glass covers the following key areas:
- Tissue integration monitoring: Histological sections at defined time points (typically 4, 8, and 12 weeks) assess fibrous encapsulation, new bone formation, and vascularisation around the implanted glass specimen.
- Inflammatory response grading: Scoring systems such as the ISO 10993-6 semi-quantitative scale classify the tissue reaction from minimal to severe, providing a regulatory-ready dataset.
- Ion release and local pH tracking: Soluble glass systems release silicate, calcium, and phosphate ions into surrounding tissue. Monitoring local pH prevents unintended acidification or alkalisation that could compromise cell viability at the implant site.
- Functional endpoint assessment: For bone-contact applications, mechanical push-out tests and micro-CT imaging quantify osseointegration strength and new bone volume.
- Correlation with in vitro data: Results that diverge significantly from in vitro predictions indicate either an inadequate cell model or a dynamic biological variable not captured in the bench assay.
The most common pitfall in translating in vitro results to in vivo outcomes is underestimating the role of protein adsorption at the glass surface. Serum proteins coat the glass within seconds of implantation, fundamentally changing the surface chemistry that cells encounter. This is why surface treatment and coating selection, covered in the previous section, directly influence in vivo performance as much as they influence bench test results. Reviewing quality standards in glass manufacturing provides additional context on how these validation stages align with regulatory submission requirements.
Key takeaways
Ensuring biocompatible glass requires a sequential process of composition selection, surface activation, multi-assay in vitro screening, and in vivo validation aligned with ISO 10993 and ASTM F756 standards.
| Point | Details |
|---|---|
| Start with composition | Select glass formulations with documented ion release profiles matched to the intended biological environment. |
| Activate before coating | Plasma treatment creates hydroxyl groups that prevent hydrophilic coating delamination in biological fluids. |
| Use multi-parametric assays | Combine MTT, LDH, and fluorescence microscopy to avoid false positives or negatives in cytotoxicity screening. |
| Test dynamically | Dynamic fluid conditions produce more accurate bioactivity data than static immersion for soluble glass systems. |
| Confirm with in vivo data | Large animal model studies are required to validate tissue integration and long-term safety before clinical use. |
Why surface treatment is the step most QA teams underestimate
Working closely with manufacturing teams across medical device and industrial sectors, I have seen the same failure pattern repeat itself. Teams invest heavily in glass composition selection and biological testing protocols, then treat surface preparation as a box-ticking exercise. The result is coating delamination in accelerated ageing tests, failed haemocompatibility data, and costly rework cycles.
The uncomfortable truth is that surface treatment is the highest-leverage intervention in the entire biocompatibility validation process. A perfectly formulated glass with a poorly activated surface will fail biological testing. A modestly formulated glass with a well-characterised, plasma-activated surface and the right polymer coating will pass. I have seen this play out in bone-contact device programmes and in diagnostic glass components where protein adsorption was the critical failure mode.
My strong recommendation is to treat surface characterisation as a formal quality gate, not a pre-production note. Contact angle measurement and XPS analysis should generate documented, traceable results before any coating is applied. Multi-disciplinary collaboration between materials scientists and cell biologists at this stage catches problems that neither discipline would identify working alone. The future of bioactive glass testing will involve more dynamic, physiologically relevant assay conditions. Teams that build dynamic testing into their standard protocols now will face fewer surprises when regulatory bodies request it.
— Alexandra
Precision Glasses: your partner for biocompatible glass manufacturing
Producing glass that meets biocompatibility requirements demands more than good materials. It demands meticulous fabrication, documented surface treatment processes, and quality assurance protocols aligned with ISO 10993 and ASTM standards.

Precision Glasses brings together advanced glass fabrication expertise and rigorous quality assurance capabilities to support manufacturers in medical devices, defence, aerospace, and industrial sectors. Our technical glass solutions are tailored to meet the specific surface, composition, and coating requirements that biocompatibility validation demands. From plasma activation through to final inspection, our quality assurance processes are built to give your QA team the documented evidence it needs for regulatory submissions. Contact Precision Glasses to discuss your biocompatible glass requirements.
FAQ
What is biocompatible glass?
Biocompatible glass is a glass material that performs its intended function without causing harmful biological responses, such as cytotoxicity, inflammation, or tissue damage, in the surrounding environment.
How do you test glass biocompatibility?
Biocompatible glass testing methods include MTT and LDH cytotoxicity assays at 24 and 48 hours, fluorescence microscopy for morphological assessment, and in vivo implantation studies in large animal models per ISO 10993.
Why is surface treatment critical for biocompatible glass?
Glass is chemically inert, which prevents coatings from bonding reliably without prior activation. Plasma treatment generates reactive hydroxyl groups that create covalent bonds with hydrophilic polymers, preventing delamination in biological environments.
What standards govern biocompatibility in glass materials?
ISO 10993-5 covers cytotoxicity testing, ISO 10993-6 covers implantation assessment, and ASTM F756 governs haemolysis testing. These are the primary regulatory frameworks for ensuring glass biocompatibility in medical device applications.
What is the difference between static and dynamic biocompatibility testing?
Static testing immerses glass in fluid without flow, which can overestimate ion accumulation at the surface. Dynamic testing simulates physiological fluid movement and produces more accurate bioactivity and ion release data for soluble glass systems.


